65 year old male with CVA
I've been given this case to solve in an attempt to understand the topic of "patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations, and come up with a diagnosis and treatment plan.
Following is the view of my case
CASE PRESENTATION
A 65 old male presented to opd with the chief complaints of
-- slurring of speech
-- difficulty in walking
-- weakness of left upper limb since yesterday
-- complain of pedal edema .
History of present illness

No association with pain abdomen,no mucus in stool
No blood in stool
History of fever 2 episodes in the past 6 months
No history of nausea vomiting
No history decreased appetite
History of past illness
K/c/o Hypertension from 7 years telma H prescribed for hepertension
N/K/C/O diabetes mellitus ,epilepsy,tuberculosis
H/o trauma 1 month back (slip and fell in bathroom)
H/o surgery 18 years back for hernia
H/o acute ischemic stroke
personal history
Married
Diet : mixed
Decreased appetite
Bowel irregular
Micturition normal
No known allergies
Addictions : habit of alcohol consumption daily
No similar complaints in the family
General examination
Done after obtaining consent , in a well lit room ,in the presence of an attendent ,with adequate exposure
The patient is conscious incoherent and incoperative ,poorly nourished
Pallor is present
No icterus,cyanosis ,koilonychia
History of pedal edema
Pedal edema is non pitting type and extending upto feet
Vitals
BP 130/70 mmhg
PR 80bpm
RR 16 cycles per min
Temperature : afebrile

SYSTEMIC EXAMINATION
Respiratory system
Inspection
Chest is normal bilaterlly symmetrical
Position of trachea is normal
No scars , sinuses or visible pulsations
palpation
All inspectory findings are confirmed
No local rise in temperature
No tenderness
Cvs
Inspection :
No visible engorged veins, scars or sinuses on chest
Palpation :S1 amd S2 are heard
No thrills or murmers
Percussion : heart borders are appreciated
Auscultation :
No cardiac murmers are heard
Abdomen
Inspection :
Umbilicus : central inverted
Soft and non tender
Palpation :
No local rise in temperature
No organomegaly
Free fluid no
No bruits
Liver and spleen are not palpable
Percussion :
Resonant
CNS
TONE : UL LL
N N
hypo N
Higher mental functions
- Conscious +
- Oriented to time+,place+ and person+
- Memory - intact
- Speech - slurred
MOTOR SYSTEM:
TONE UL. N. Left hypotonia
LL. N. N
POWER
a) neck muscles
b) UL
•shoulder
•Elbow
•Wrist 0/5
• Small muxles & hand
Hand grip
c) LL
•Hip
. Knee
Ankle
Small musles
(d) Trunk muscle
REFLEXES.
a)
A superficial.
corneal. ++
Conjunctival. ++
Pharyngeal ++
Palatal. ++
Sensory SYSTEM
Test
I-SPINOTHALAMIC Right Left
1. Crude touch. ++
2. Pain++
3. Temperature++
II POSTERIOR COLUMN
1.fine Touch++
2. Vibration++
3. Position sense++
III CORTICAL
1. Two point discrimination++
2. Tactile localisation++
3 Graphaesthesia+
Cranial nerve examination
1olfactory sense - normal
2- visual acuity present,
R L
Direct reflex +. +
Indirect reflex + +
3,4,6 - no ptosis Or nystagmus
5- corneal reflex present
7- deviation of mouth, no loss of nasolabial folds, forehead wrinkling present
8- Normal
9,10- position of uvula is central
11- sternocleidomastoid contraction present
12- deviation of tongue
Investigations












19/01/2023
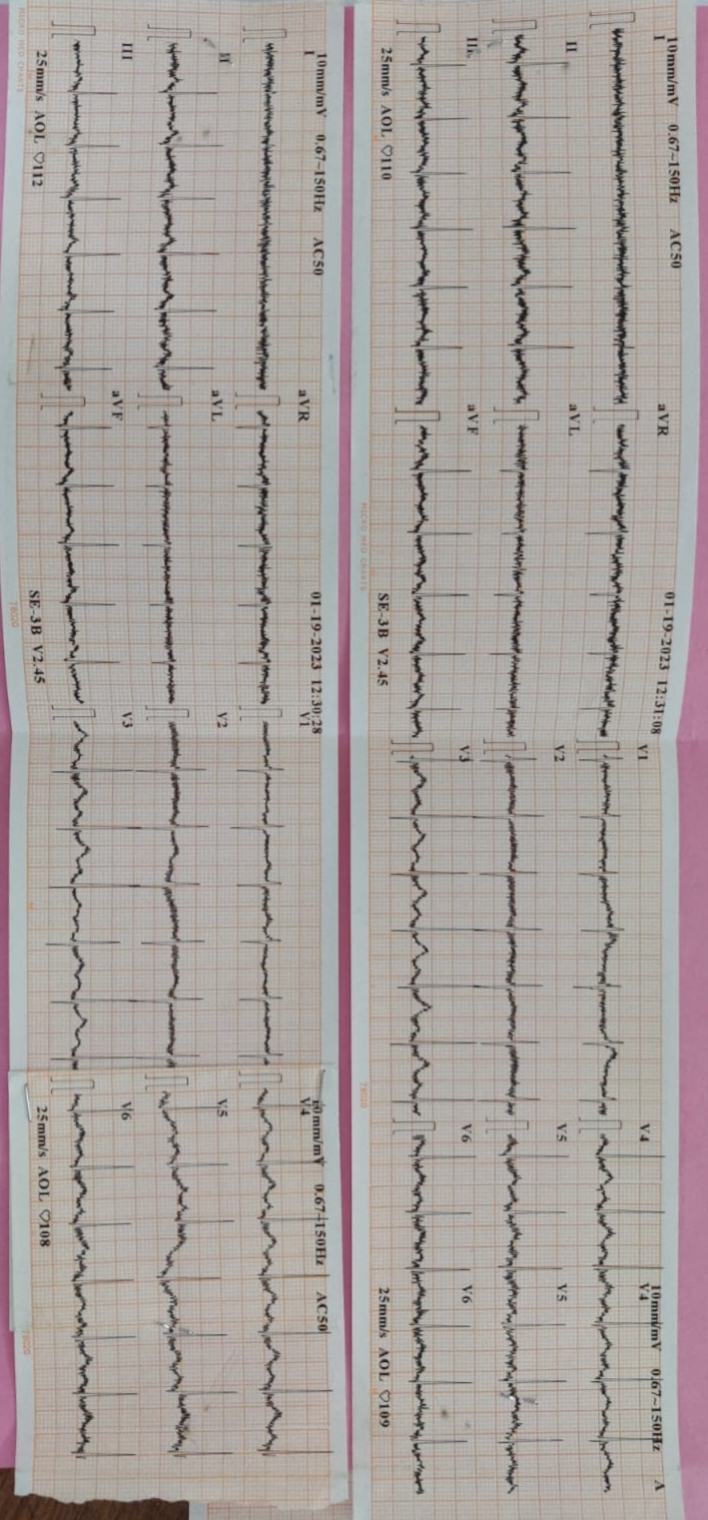





Clinical images


Provisional diagnosis :
Cerebro vascular accident with hyperacute infarts and hypertension
Treatment
Tab clopidogrl 75 mg OD
Tab ecospirin 75 mg OD
Tab atarvostat 20 mg OD
Tab telma
Tab telmesartan 40 mg OD





Comments
Post a Comment